Table of Contents
Hyperkalemia can be classified as mild, moderate and severe as well as acute and chronic.
Severe hyperkalemia will be acute as it will require immediate treatment.
This article will address treatment strategies based on the severity of hyperkalemia.
Treatment of Hyperkalemia
Treatment Options
Stabilization of cardiac cell membrane
Redistribution from extracellular to intracellular space.
Remove potassium from body
Address Causes of Hyperkalemia
Diet
Approach to Treatment
Mild Hyperkalemia: K < 5.5
Causes of hyperkalemia are reviewed here:
High K – What’s the Deal? How to think about Hyperkalemia | BCNephro
Hyperkalemia severity:
- Mild: < 5.5 mmol/L
- Moderate: 5.5-6.5 mmol/L
- Severe: > 6.5
In my opinion and experience the risk for cardiac arrhythmias is only significant with severe hyperkalemia.
Hyperkalemia Acute vs Chronic:
Acute:
- Cellular shifts major factor
- More likely to be severe
- Requires urgent treatment
Chronic:
- Decreased renal excretion main factor
- More likely to be mild-moderate
- Less urgent, but ongoing treatment required
Treatment Options
Treatment of hyperkalemia in order from most severe/urgent includes:
- Stabilization of cardiac cell membrane
- Redistribution from extracellular to intracellular space
- Elimination of potassium from the body
- Removal of medication causes of hyperkalemia
- Dietary potassium restriction
Stabilization of cardiac cell membrane
This is done with intravenous calcium
- Calcium chloride – 10 ml of 10% solution over 2-5 minutes
- Calcium gluconate 30 ml of 10% solution over 2-5 minutes
- Effect lasts 30 – 60 minutes
- Avoid if digoxin toxicity: Digitalis works by impairing the Na/K ATPase creating an electrochemical gradient for calcium to enter the cell. Digoxin toxicity may cause hyperkalemia, complete paralysis of the Na/K ATPase prevents potassium from entering the cell. In this situation the electrochemical gradient for calcium to enter the cell is very high and providing intravenous calcium may precipitate a cardiac arrhythmia.
Redistribution from extracellular to intracellular space.
Potassium can be driven from the extracellular to intracellular space by the following:
- Insulin/ dextrose:
- Insulin:
- 10 units IV
- Effect occurs in 10-20 minutes
- Effect lasts 4-6 hrs
- Dextrose to mitigate hypoglycemia (given unless BG < 250)
- 25 grams IV dextrose push
- If BG < 126 give additional D10 @ 50 ml/ hr x 5 hrs
- Insulin:
- Albuterol:
- Given via nebulizer
- Sodium bicarbonate
- Only effective if there is an associated metabolic acidosis
Remove potassium from body
This can be done via enhancing renal excretion, extrarenal (GI excretion), or extracorporeal removal (dialysis).
- Renal excretion
- Kaliuresis be induced with a combination of sodium (NS) with a loop diuretic
- Diuretic
- Thiazide if HTN
- Loop if edema
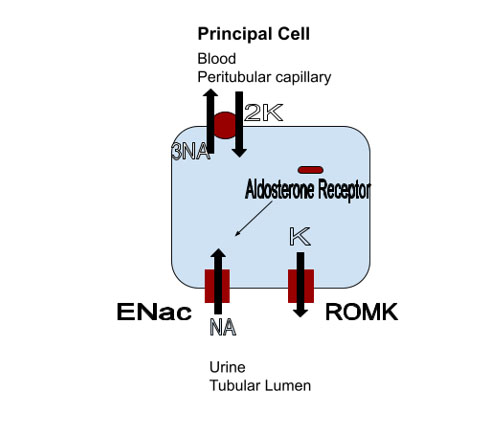
- Fludrocortisone
- Mineralocorticoid agonist
- Use if no HTN or edema
- Extrarenal: GI elimination
- Sodium polystyrene sulfonate (Kayexalate)
- Site of action: Colon
- Associated with intestinal necrosis
- Patiromer (Veltassa)
- Site of action: Colon
- Sodium zirconium cyclosilicate
- Site of action: Small and large intestines
- Acute: 10 grams 3 times daily for 6 doses
- Chronic: 5 grams every other day – 15 mg daily
- Sodium polystyrene sulfonate (Kayexalate)
- Extracorporeal: Dialysis
- Potassium concentration decreases
- 1 mmol/Liter 1st hour
- Then 1 mmol/Liter over next 2 hours
- Potassium concentration decreases
Address Causes of Hyperkalemia
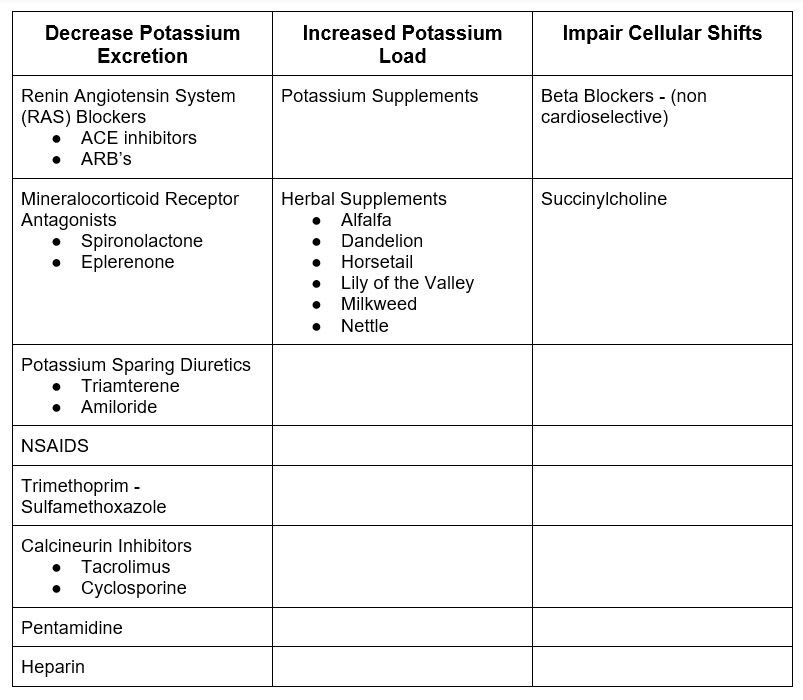
Medications: May cause hyperkalemia by different mechanisms
Diet
Diet is rarely the sole cause of hyperkalemia. However it can exacerbate another predisposing cause of chronic hyperkalemia with impaired potassium excretion.
Approach to Treatment
My approach to treatment of hyperkalemia is based on severity with the understanding that severe hyperkalemia is most likely related to cellular shifts. Treatments that are based on cellular shifts of potassium will only be temporarizing. This will not be practical for management of chronic hyperkalemia.
Mild K < 5.5
- Decrease Potassium Intake
- Avoid / Moderate high potassium foods
- Discontinue potassium supplements
- Increase Potassium Excretion
- Add diuretic if indicated
- HTN – thiazide
- Edema – loop
- Add diuretic if indicated
Mild-Moderate K 5.5 – 6.0
- Decrease Potassium Intake
- Avoid / Moderate high potassium foods
- Discontinue potassium supplements
- Increase Potassium Excretion
- Add diuretic if indicated
- HTN – thiazide
- Edema – loop
- Hold or decrease doses of medications that decrease renal potassium excretion
- Consider potassium binding agent if compelling indication for medication that impairs renal potassium excretion (i.e. RAS blocker)
- Add diuretic if indicated
- Cellular Shifts
- Add Sodium Bicarbonate if chronic metabolic acidosis
Moderate-Severe K 6.0 – 6.5
- Stabilize cell membrane (If EKG changes)
- Calcium Gluconate
- Decrease Potassium Intake
- Avoid / Moderate high potassium foods
- Discontinue potassium supplements
- Increase Potassium Excretion
- Add diuretic if indicated
- HTN – thiazide
- Edema – loop
- Hold medications that decrease renal potassium excretion
- Add potassium binding agent
- Add diuretic if indicated
- Cellular Shifts
- Add Sodium Bicarbonate if chronic metabolic acidosis
Severe > 6.5
- Stabilize cell membrane
- Calcium Gluconate
- Cellular Shifts
- Insulin/Dextrose
- Albuterol Nebulizer
- IV Bicarbonate (if metabolic acidosis)
- Decrease Potassium Intake
- Avoid / Moderate high potassium foods
- Discontinue potassium supplements
- Increase Potassium Excretion
- Saline and/or loop diuretic
- Hypovolemia: Saline
- Euvolemia: Saline + loop diuretic
- Hypervolemia: Loop Diuretic
- If refractory (especially if oligoanuric)
- Hemodialysis
- Hold medications that decrease renal potassium excretion
- Add potassium binding agent
- Saline and/or loop diuretic
Summary
Treatment of Hyperkalemia can entail numerous physiological approaches including:
- Stabilization of cardiac cell membrane
- Redistributing potassium from extracellular to intracellular space
- Enhanced elimination from the body.
The severity and acuity of hyperkalemia will guide which treatments should be undertaken.
{kind=link}
{kind=link}
{kind=link}