Table of Contents
What happens if you only have one kidney?
Causes of a Solitary Kidney
First, what are the reasons that someone would have only one kidney? These can be broken down to congenital or acquired.
Congenital
Some are born with only one or one functional kidney. This can be because:
- The kidney never formed (renal agenesis)
- The kidney never developed (renal aplasia)
- A nonfunctional kidney developed: multicystic dysplastic kidney.
It is difficult to definitively distinguish renal agenesis from renal aplasia. Aplastic kidneys may subsequently involute and be absent on imaging. Approximate incidences are:
- Unilateral Renal Agenesis: 1 in 2000 births.
- Unilateral Renal Aplasia: 1 in 1300 births.
- Unilateral non functioning kidney: multicystic dysplastic kidney: 1 in 4300 births.
With these congenital abnormalities there is an increased incidence of abnormalities in the solitary kidney or urinary tract. A Congenital Abnormality of the Kidney or Urinary Tract (CAKUT) is present in approximately ⅓ of these patients.
To learn more about congenital solitary kidney check out this article. Clinical Implications of the Solitary Functioning Kidney
Reasons for Solitary Kidney
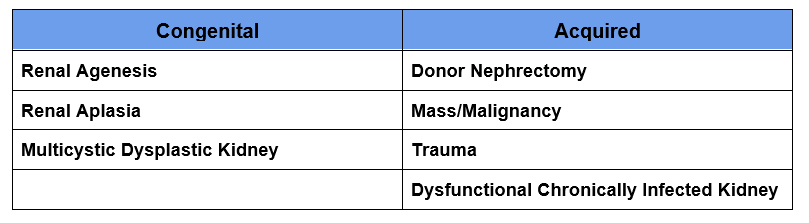
Acquired
This is when one kidney is removed. A kidney may be removed because of:
- Malignancy
- Kidney donor
- A nonfunctional/dysfunctional kidney with complications (such as infection)
- Trauma
Kidney Function with a Solitary Kidney
What happens with one kidney? The logical assumption is that the kidney function will decrease by half. Lose 50% total kidney mass end up with 50% total kidney function. This is not necessarily the case. It depends if the other kidney is normal.
We are born with approximately 900,000 nephrons in each kidney. Although it is true that nephrogenesis, the production of new nephrons does not occur after birth, the remaining nephrons have the ability to compensate by hyperfiltration.
Remaining Kidney is Normal
The best example of this is a donor nephrectomy. Someone should not be accepted as a kidney donor if the remaining kidney is not normal. In these cases the remaining kidney hypertrophies to compensate for the decreased renal mass. This has been studied. The GFR of the solitary kidney reaches:
- 70% of the pre nephrectomy GFR within 2-3 weeks
- 75% – 85% of pre nephrectomy GFR long term
- eGFR increased by 1.47 ml/ minute per year between 6-36 months (compared to the normal decrease in GFR of 0.36 ml/minute per year in controls)
A congenital solitary kidney may develop more nephrons than a typical kidney, but it will still be less than 2 normal kidneys. If it is normal, it will also hypertrophy and develop a GFR that is more than 50% and result in a creatinine in the normal range.
Assuming the normal solitary kidney has 80% of a normal total GFR.
Normal GFR 125 ml/minute x 80% remaining GFR 100 ml/minute
This will be associated with a serum creatinine in the normal range.
This compensatory hypertrophy can be seen on imaging, typically the kidney is enlarged on ultrasound.
Remaining Kidney is Abnormal
Patients who require a nephrectomy for another reason, such as malignancy, may be left with a solitary kidney that is not normal. If there is a decreased GFR (CKD) at baseline then neither kidney is normal. We have established that one normal kidney should compensate enough to achieve a GFR in the normal range.
In these cases I do not anticipate compensatory hypertrophy. I predict there will be a decrease in kidney function post nephrectomy. However, the decrease may not be 50%. The kidney that is removed may be more severely abnormal and contribute less than 50% of the total function.
A nuclear medicine split renal function scan will estimate the percent of function that each kidney is contributing.
This is not the function of each kidney, it is the percent of total function (whatever that is) that comes from each kidney. The numbers will always add up to 100%. This may be important to clarify to patients.
I take the percent split function of the remaining kidney and multiply it by the pre nephrectomy total GFR to predict the post nephrectomy GFR.
Example:
Pre nephrectomy GFR: 50 ml/minute
Split Renal function 70% (remaining kidney) 30% (kidney to be removed)
Predicted post nephrectomy GFR: 50 ml/minute x 70% = 35 ml/minute
Long term Risks of a Solitary Kidney
Remaining Kidney is Normal
Post Donor Nephrectomy
The long term renal outcomes of kidney donors are excellent, but there are some risks.
- The risk of kidney failure (ESRD) is very low, lower than the general population. However, it is higher than if they had not donated
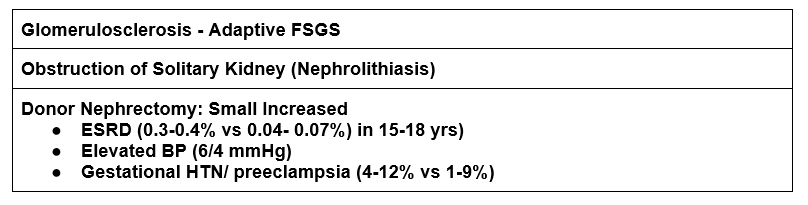
- One study determined the risk of ESRD was 0.47% for kidney donors vs 0.07% developing at a median 18.7 yrs
- Another study found an incidence of 30.8 per 10,000 pts (0.308%) vs 3.9 per 10,000 (0.039%) patients at 15 years
- The blood pressure is slightly higher (by 6/4 mmHg)
- Increased risk of gestational HTN (4-12% vs 1-9%) and preeclampsia (4-10% vs 1-3%)
- There is slightly higher urine albumin excretion.
Hyperfiltration
With a solitary kidney, either congenital or acquired, the nephron number is reduced. The remaining nephrons do more work to help preserve the GFR. Therefore, they are subject to more stress. This is hyperfiltration and may be maladaptive resulting in glomerulosclerosis. This leads to further hyperfiltration of the remaining good nephrons and a vicious cycle ensues.
A manifestation of glomerulosclerosis from hyperfiltration is proteinuria. This should be screened for and treated with Renin Angiotensin System blockers and other agents. HTN should also be treated aggressively.
Although a congenital solitary kidney may have produced more nephrons before birth, there still is risk as hyperfiltration occurs for a longer time, since birth.
Risks of Solitary Kidney
Remaining Kidney is Abnormal
If the remaining solitary kidney is abnormal it would not be expected to be able to achieve a higher GFR with hyperfiltration. The result: More severe CKD.
Kidney stones
Although kidney stones are not caused by a solitary kidney, the implication of a kidney stone passage is that it may cause AKI. Typically when a stone is causing obstruction the contralateral kidney will pick up the slack until it passes. This cannot occur if there is only one kidney.
Summary
There are many reasons for a solitary kidney, both congenital and acquired. In many cases the solitary kidney is normal and compensates achieving a GFR of up to 85% that of two normal kidneys. In some cases this hyperfiltration can be maladaptive leading to glomerulosclerosis manifest by proteinuria. In addition to monitoring of kidney function, patients with a solitary kidney should be monitored for hypertension and proteinuria. If present these should be aggressively treated.



{kind=link}
{kind=link}
{kind=link}