Table of Contents
What is a Renal Scan?
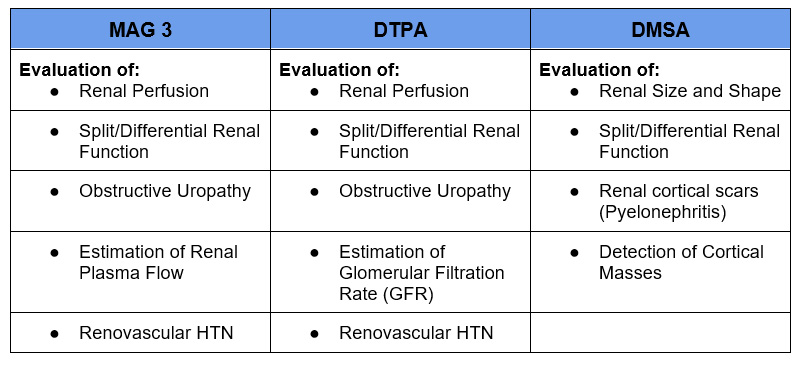
A nuclear medicine renal scan involves imaging with a compound taken up by the kidney that is bound to a radioisotope. There are different compounds used that are bound to the radioisotope technetium:
- MAG3: 99m dimercaptosuccinic acid
- Most common compound used for renal scans
- Rapid extraction by renal tubular cells. Higher extraction rate than DTPA.
- Secretion is mainly by proximal tubules
- DTPA: 99m diethylene triamine penta-acetic acid
- Second most common compound used for renal scans
- Primarily cleared by glomerular filtration
- DMSA: 99m dimercaptosuccinic acid
- Less commonly used
- Binds to renal tubules
- Used to image renal parenchyma (cortex) due to its prolonged retention.
Uses of Different Compounds in Renal Scan
Radionuclide renal scan involves radiation exposure, significantly more than an X-ray, but significantly less than a CT scan. For this reason it is contraindicated in pregnancy.
Indications for Renal Scan
Radionuclide renal scans are less commonly used. Alternate imaging, particularly with CT or MR, has become more common. However, there still is important information that can be obtained from these scans. Most often this is for the evaluation of obstructive uropathy and assessment of split or differential renal function.
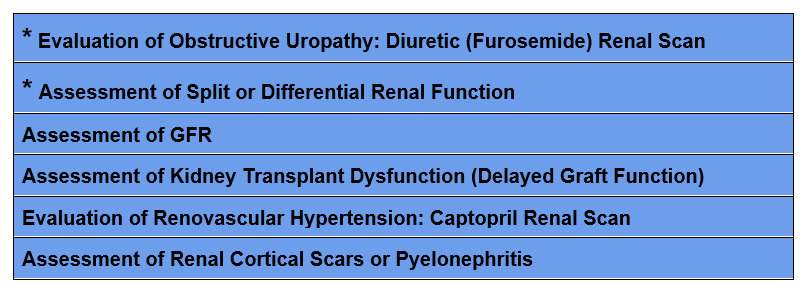
*Common Uses
Evaluation of Obstructive Uropathy: Diuretic (Furosemide) Renal Scan
Renal scanning is often used to assess if hydronephrosis is due to true functional obstruction as opposed to anatomic non-obstructive dilatation. Non obstructive hydronephrosis can be seen in vesicoureteral reflux, congenital malformations, or with a noncompliant bladder.
In these cases a diuretic (furosemide) renal scan is performed.
- The radionuclide (typically bound to MAG3) is injected.
- Renal excretion of the radiotracer is assessed.
- Diuretic (furosemide) is administered.
- If radiotracer excretion increases (normal half life < 9.8 minutes), indicative of non obstructive dilatation.
- If radiotracer excretion unaffected or minimally effective (prolonged half life > 20 minutes) consistent with obstructive uropathy
- NSAIDS should not be administered as affect radionuclide excretion
Split Differential Renal Function
There are times when it may be important to know how much function each kidney is contributing. This is particularly important pre nephrectomy to determine if the remaining solitary kidney has sufficient function. Normally each kidney will contribute close to 50%, but this may not be the case if one kidney is diseased or has a congenital malformation.
- Can be done with MAG 3 or DTPA
- If DTPA used can also get an assessment of glomerular filtration rate (GFR)
- Shows relative not absolute kidney function. The numbers will always add up to 100%. It is often necessary to counsel patients on this.
Example: If a patient has a unilateral atrophic kidney and the split differential scan is 75% – 25%. The patient may instinctively think that their “bad” kidney has 25% function and their “good” kidney also is not normal, only has 75% function.
- An estimate of GFR is necessary to determine absolute kidney function
Living with One Kidney – The Solitary Kidney @BCNephro
The Solitary Kidney: Living with One Kidney | BCNephro
Estimation of GFR
As DTPA is excreted by glomerular filtration it can give an estimate of GFR when used for the split differential renal scan.
This is not commonly done as GFR is more often assessed by:
- Creatinine
- Cystatin C
- 24 hour urine creatinine clearance
Creatinine Cystatin C and GFR @BCNephro
Creatinine, Cystatin C and GFR BCNephro
However, there are situations such as in evaluation of living kidney transplant donors where a renal scan may be used to confirm GFR.
Evaluation of Kidney Transplant Delayed Graft Function
Renal scanning with MAG 3 or DTPA (MAG 3 preferred) can be used to assess delayed graft function of renal transplants in the early postoperative course.
There are multiple causes of delayed graft function that need to be distinguished.
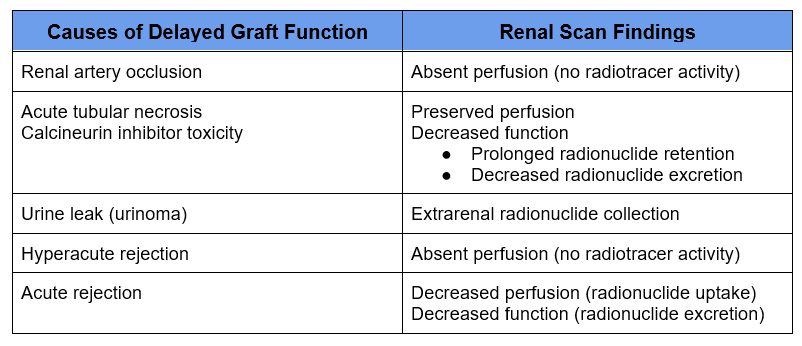
Renal scan is not commonly done in this context. Evaluation for technical (renal artery or urine leak) is more often assessed with doppler renal ultrasound. Biopsy is used to definitively distinguish acute rejection and acute tubular necrosis.
Evaluation for Renovascular Hypertension: Captopril Renal Scan
This involves renal scanning after administration of an angiotensin converting enzyme (ACE) inhibitor, typically captopril. Also referred to as a Captopril Renal Scan. MAG 3 is preferred radionuclide, although DTPA can be used.
- Rarely done in current clinical practice. CT angiography (CTA) or MR angiography (MRA) are typically the tests of choice for evaluating renal artery stenosis.
- Assess renal perfusion and excretion after administration of an ACE-I (Captopril)
- Decreased perfusion (unilateral kidney uptake < 40% of total) suggests hemodynamically significant (60-90%) renal artery stenosis.
- Has 90 % sensitivity and specificity if kidney function (baseline GFR) is normal.
- Only useful in diagnosis of unilateral (not bilateral) renal artery stenosis.
- ACE inhibitors (or other renin angiotensin system blockers) need to be held, typically for one week.
Evaluation of Kidney Morphology
DMSA has significant and prolonged uptake in the renal cortex
- Used to assess renal cortical scarring and pyelonephritis (particularly in pediatrics)
- Largely replaced by other imaging (i.e. MRI)
Summary
Although alternate imaging has replaced many uses for nuclear medicine radionuclide scan, there still is an important role for this imaging. Renal scan may be particularly useful in the evaluation of obstructive uropathy, split or differential renal function prior to nephrectomy and as an alternative way to assess GFR.
For more information check out the following links:
ACR–SPR Practice Parameter for the Performance of Renal Scintigraphy
Nuclear Renal Scan – StatPearls – NCBI Bookshelf



{kind=link}
{kind=link}
{kind=link}