Table of Contents
When writing this article I felt a need to add more and more information, to be comprehensive. I had a fear of leaving something out.
I need to stop. The intention of BCNephro is not to be an encyclopedic nephrology resource.
The intention is to share my experiences in a way that makes topics in nephrology easy to understand.
This is where the 80-20 (Pareto) principle comes in.
What is the Pareto principle?
80% of outcomes come from 20% of causes
How does this apply to immunosuppression in kidney diseases? If you know the following 5 immunosuppressive medications you will know the vast majority of treatments for glomerulonephritis and glomerulopathies (nephrotic syndrome). After these 5 there are diminishing returns.
Immunosuppression: The Big 5
- Glucocorticoids
- Cyclophosphamide
- Calcineurin inhibitors
- Rituximab
- Mycophenolate Mofetil
Glucocorticoids
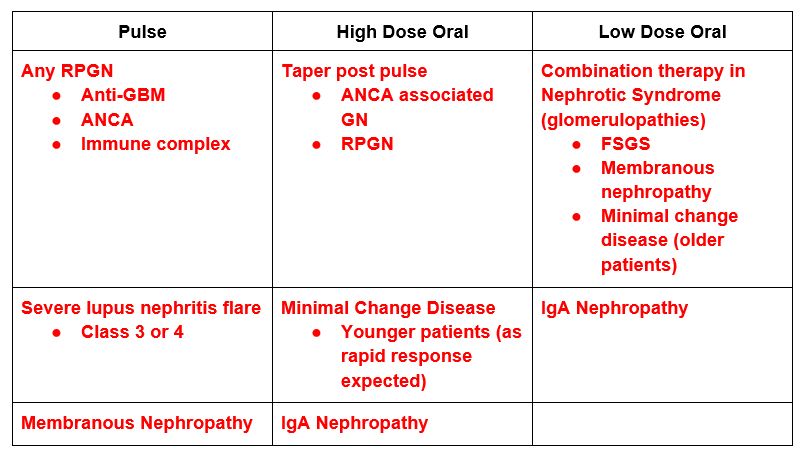
Dosing: Glucocorticoids are typically given in 2 ways
- IV: Pulse methylprednisolone. 1 gram daily x 3 days
- Oral: Prednisone.
- High dose: (ie. 60 mg a day or 120 mg every other day) used in:
- Taper post IV pulse
- Single agent therapy
- Low Dose: (ie. 15 mg day or ½ mg/kg every other day)
- In conjunction with other immunosuppressants
- High dose: (ie. 60 mg a day or 120 mg every other day) used in:
Things to be Aware of:
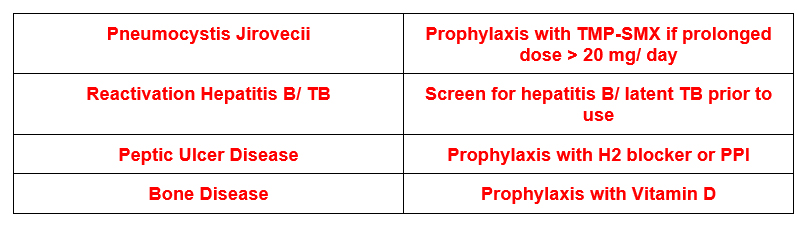
When I Use:
My take:
- I will not use high dose prednisone for > 2 months. Patients will universally become Cushingnoid and often have severe complications.
- I prefer regimens with low dose steroids in combination with other immunosuppressants.
Cyclophosphamide
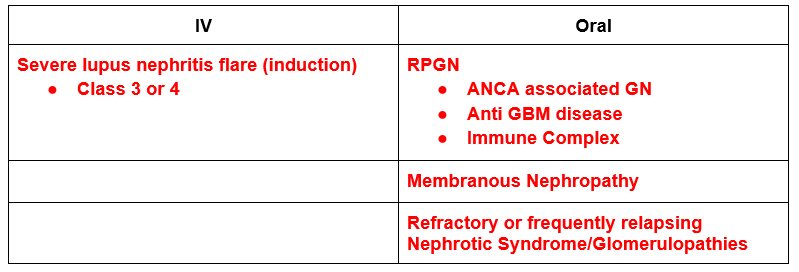
Dosing: Cyclophosphamide also can be given IV or PO
- IV
- 750 mg / m² monthly
- 500 mg (flat dose) every 2 weeks
- Oral – 1.5-2 mg / kg
Things to be Aware of:
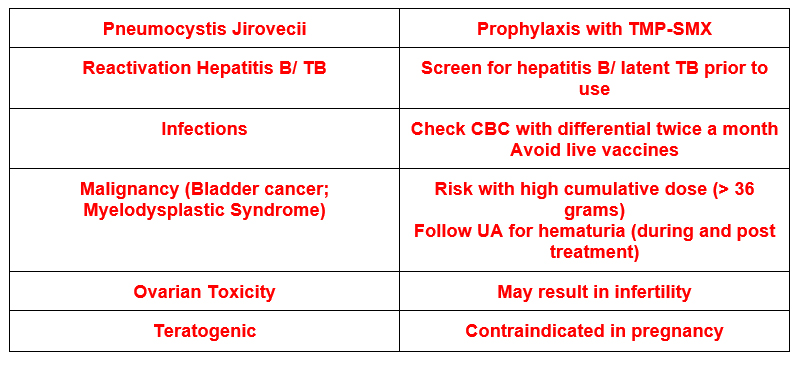
When I Use:
My Take:
- Avoid prolonged use (> 6 months oral or multiple IV courses).
- More likely to induce durable remission than other immunosuppressants (especially calcineurin inhibitors)
- Useful agent despite concerns of toxicities leading to preferential use of other agents
- Avoid use in elderly or frail patients
- Prefer to start with lower doses (ie 1.5 mg/kg/day oral). Decrease dose further with decreased eGFR or elderly
Calcineurin inhibitors: Cyclosporine and Tacrolimus
Dosing:
Oral:
- Cyclosporine:
- 3-5 mg/kg/day divided in two daily doses (every 12 hrs)
- Target Trough: 150-200
- Tacrolimus:
- 05 – 0.10 mg/kg/ day – divided in two daily doses (every 12 hrs)
- Target Trough: 4-7
Things to be Aware of:
When I Use:
My take:
- Frequent relapse when weaned.
- Prolonged course (1-2 years) with slow wean.
- Membranous Nephropathy: useful as bridge therapy with rituximab.
- FSGS: My preferred option with low dose steroids.
Rituximab
Dosing:
- IV: Typically given in 2 doses (1 gram separated by 2 weeks)
- Can also give 375 weekly x 4 (which is the standard lymphoma dose)
- Maintenance can be dosed every 6 months
Things to be Aware of:
When I Use:

My Take:
- Often preferred over cyclophosphamide (especially in elderly and frail patients). It is considered safer, but is by no means safe.
- Can follow CD 19 count to help decide timing of maintenance doses.
MMF: Mycophenolate mofetil
Dosing:
- Oral: Target dose 1000 – 1500 mg twice a day.
- Often start at 500 mg twice a day with uptitration as tolerated.
Things to be Aware of:
When I Use:

My Take:
- Often preferred for in SLE nephritis (over cyclophosphamide) particularly when concerns of fertility in female patients.
- Sometimes used as an attempt in other refractory or relapsing glomerulopathies.
Summary
Familiarity of the dosing, complications and indications of these 5 immunosuppressive medications will provide one with the knowledge of the treatment of the vast majority of glomerulonephritis and nephrotic syndrome glomerulopathies.



{kind=link}
{kind=link}
{kind=link}