Table of Contents
This article will provide an overview of diuretics including:
- Mechanism of action
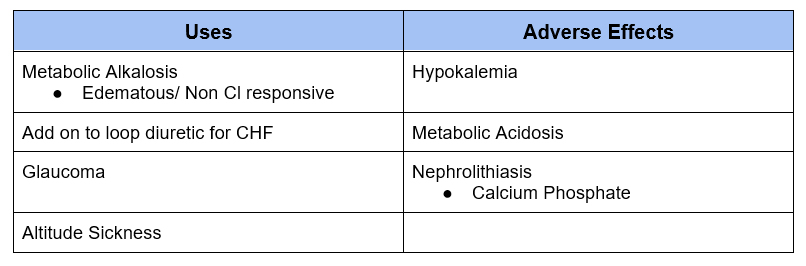
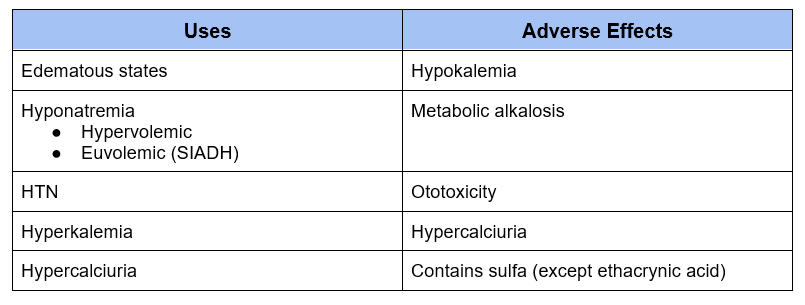
- Clinical uses
- Adverse effects
The majority of sodium that is filtered by the glomerulus is reabsorbed in the tubules. If you have normal kidney function and normal diet, less than 1% of the filtered sodium is excreted in the urine.
Diuretics impair renal tubular sodium reabsorption in different parts of the nephron. This leads to excretion of sodium and water.
Reabsorption of Sodium and Diuretic Sites of Action
- Proximal Tubule: 60-65%
- Carbonic Anhydrase Inhibitors
- Loop of Henle: 20-25%
- Loop Diuretics
- Distal Convoluted Tubule: 3-5%
- Thiazides
- Connecting Segment and Collecting Tubule: 1-2%
- Potassium Sparing Diuretics and Mineralocorticoid Antagonists
Carbonic Anhydrase Inhibitors
- Acetazolamide
- Others medication that have carbonic anhydrase effect
- Topiramate
- Zonisamide
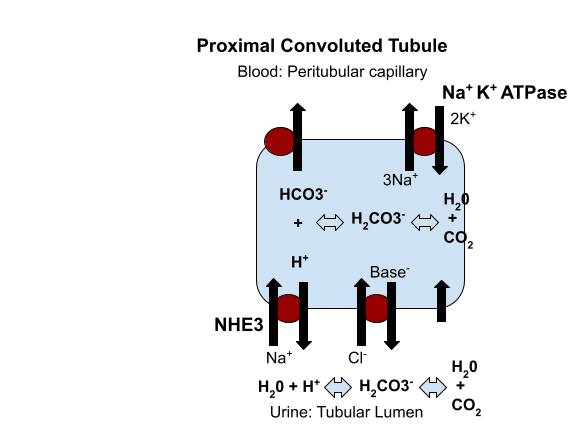
Mechanism of Action
- Blocks carbonic anhydrase
- Active in proximal tubule and to a lesser extent in distal tubule
- Carbonic anhydrase allows for conversion of H+ and HCO3– to CO2 and H20 by the following chemical reaction.
HCO3– + H+ ⇄ H2CO3 ⇄ H20 + CO2
This process is necessary to allow for Na reabsorption via the Na+H+ antiporter. It also allows for HCO3- reabsorption.
Since the proximal tubule is where the majority of Na is reabsorbed one would think that impairing it would result in the greatest diuretic effect. However, this is not the case as the majority of non reabsorbed fluid ends up being reabsorbed in more distal parts of the nephron, particularly the loop of Henle.
Loop Diuretics
- Furosemide
- Bumetanide
- Torsemide
- Ethacrynic Acid
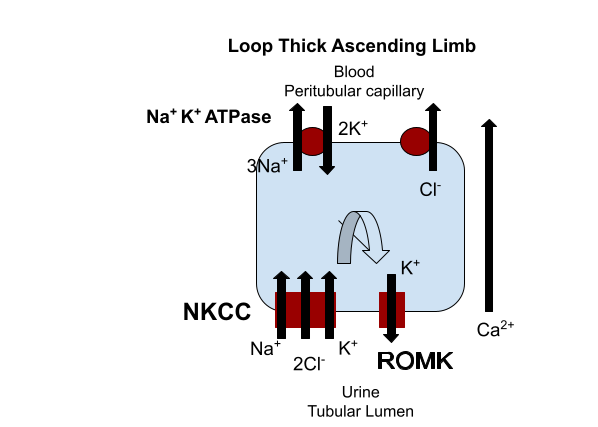
Mechanism of Action
- Blocks NKCC channel
- Thick Ascending limb of loop of Henle
- Impairs both urinary dilution (by blocking tubular Na+ reabsorption) and concentration (by impairing medullary concentration gradient)
Although only 25% of filtered sodium is reabsorbed in the Loop of Henle this class of diuretics has the greatest diuretic effect as the distal nephron has a more limited capacity to upregulate.
There is low cross reactivity between antibiotic sulfa allergy and diuretic sulfa allergy. Many patients with a sulfa allergy to antibiotics can safely take diuretics that contain sulfa.
Torsemide has a longer half life and more predictable GI absorption than furosemide. For this reason it may be more effective for congestive heart failure and hypertension.
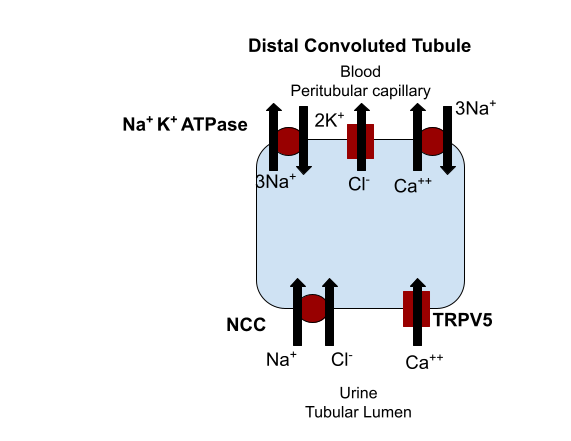
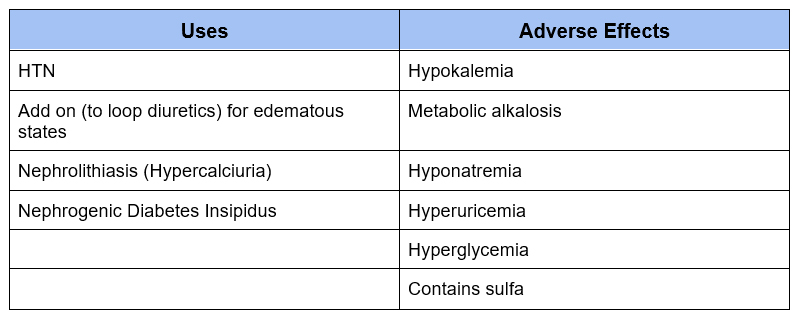
Thiazides
- Hydrochlorothiazide (HCTZ)
- Indapamide
- Chlorthalidone
- Metolazone
- Chlorothiazide (IV)
Mechanism of Action
- Blocks Na+Cl– cotransporter
- Distal Convoluted Tubule
- Impairs urinary dilution. In the cortex so does not affect urinary concentration gradient
- Increases calcium reabsorption
Chlorthalidone and indapamide have a longer half life and are more potent than hydrochlorothiazide (HCTZ).
Similar to loop diuretics there is a low cross reactivity between antibiotic sulfa allergy and diuretic sulfa allergy
Chlorthalidone is my go to for HTN and hypercalciuria
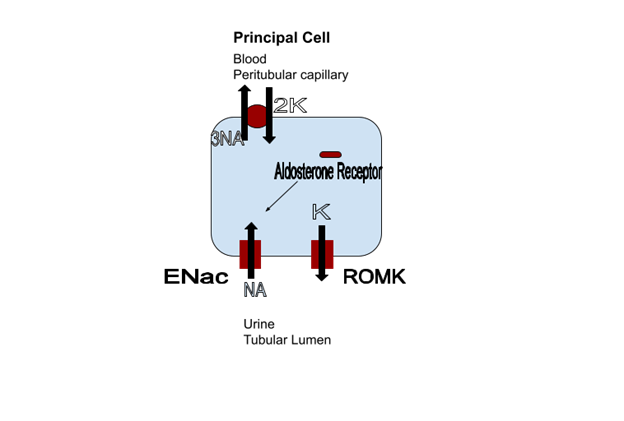
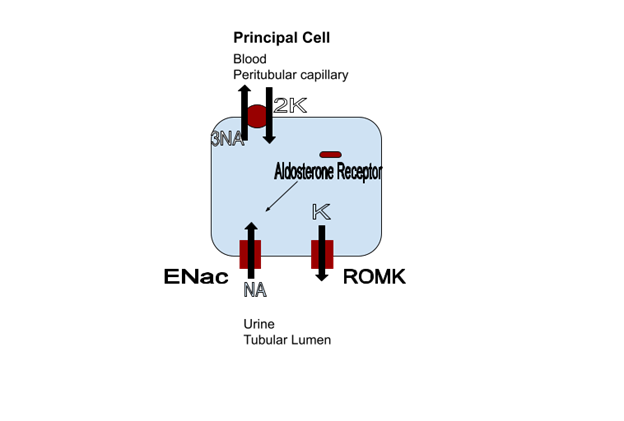
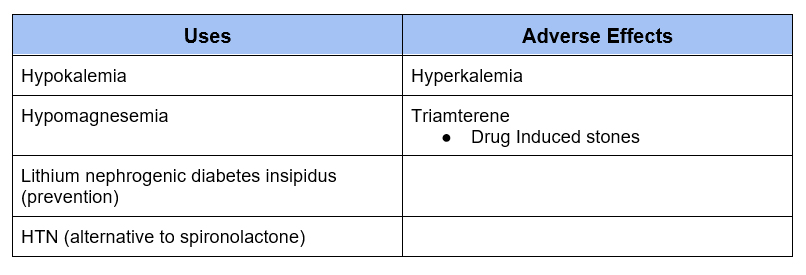
Potassium Sparing
- Triamterene
- Amiloride
Mechanism of Action
- Blocks epithelial sodium channel
- Aldosterone Sensitive Distal Nephron
- Connecting Tubule and Collecting Duct
Although triamterene is commonly found in combination with HCTZ, I prefer amiloride.
In addition to treatment of hypokalemia, amiloride is an alternative for patients who do not tolerate a mineralocorticoid antagonist.
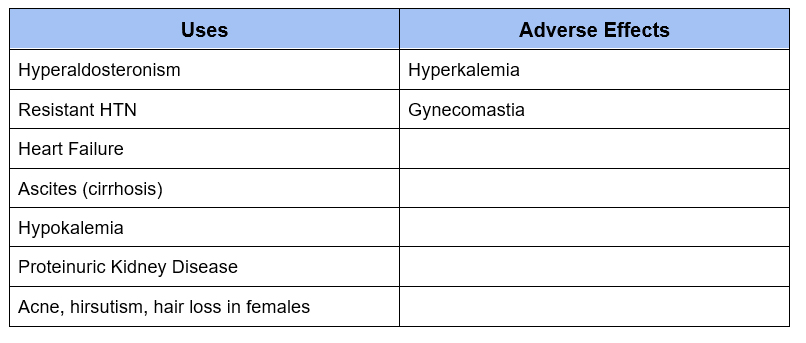
Mineralocorticoid Antagonist
- Spironolactone
- Eplerenone
- Finerenone
Mechanism of Action
- Blocks Mineralocorticoid Receptor
- Aldosterone Sensitive Distal Nephron
- Connecting Tubule and Collecting Duct
Spironolactone has cross reactivity with progesterone receptors, this is the reason for potential adverse effect of gynecomastia. I typically do not see gynecomastia at 25 mg dose
Eplerenone is specific for the mineralocorticoid receptor, but is less potent than spironolactone.
Finerenone is a non steroidal mineralocorticoid antagonist. It is purported to have a lower incidence of hyperkalemia and less of an antihypertensive effect. It is used for diabetic kidney disease.
Summary
Diuretics have their effect by blocking sodium reabsorption at different sites of the nephron. Knowledge of the site of action helps to understand clinical uses and side effects.



{kind=link}
{kind=link}
{kind=link}