Table of Contents
Is there a role for dialysis in acute liver failure?
Hepatic failure can be associated with acute kidney injury and dialysis may be indicated in these situations, that’s not what this article will address. Instead we will explore a role for dialysis in acute liver failure even if there is not kidney failure.
There may be consideration to perform dialysis to remove a toxic substance in a patient without kidney failure.
Some examples are life threatening drug intoxications.
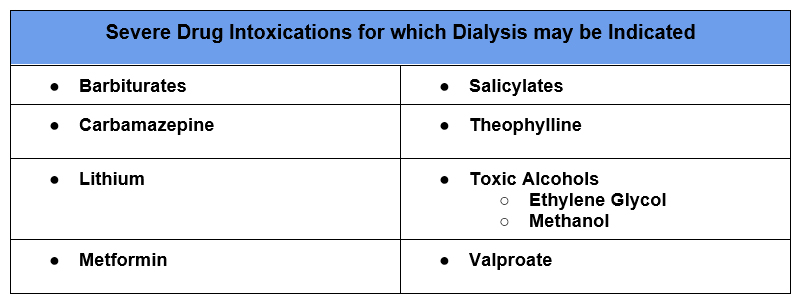
Toxic Alcohol Ingestions @BCNephro
The Extracorporeal Treatments in Poisoning Workgroup (EXTRIP) has developed recommendations for and against dialysis for many drug intoxications.
RECOMMENDATIONS | extrip-workgroup
What Criteria Determine the Efficacy of Dialysis?
The first thing we want to consider is how toxic the substance is. Is it associated with significant morbidity or mortality?
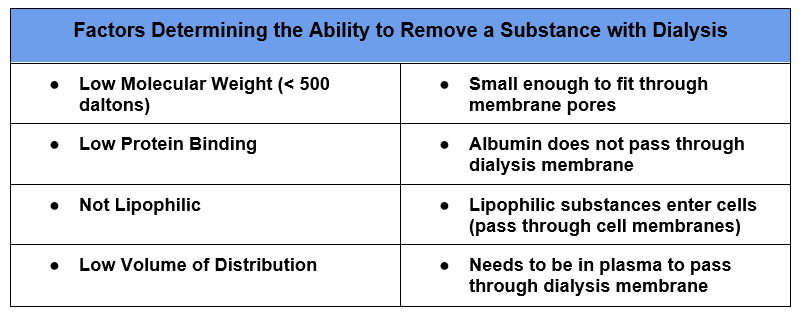
Second, can the substance be removed by dialysis?
Finally, does removing the substance with dialysis reduce this morbidity or mortality? For example, if a substance has a high endogenous clearance dialysis may offer little additional benefit.
When dialysis is used to remove substances that meet the first two criteria, but have a large volume of distribution there will be significant rebound post dialysis. In these cases prolonged (or continuous) or multiple dialysis sessions may be required.
Ammonia
Another situation where there can be a role for dialysis is a severe elevation in ammonia, hyperammonemia, which can occur in acute liver failure.
What is Ammonia?
Ammonia is a waste product of protein metabolism. It is generated from urea (another waste product), mainly in the intestine. Intestinal mucosa generates it as do bacteria in the colon. Ammonia is also produced in other cells in the body.
In the kidney ammonia is generated in the proximal tubules and is the main way of acid secretion. Ammonia (NH3) is converted to ammonium (NH4+) in the distal tubule and is excreted in the urine. Ammonia also is converted to glutamine in skeletal muscle.
However, the main way ammonia is metabolized is by the liver. The liver clears ammonia by converting it to urea via the urea cycle.
What Causes Hyperammonemia?
- Urea cycle disorders, deficiencies in enzymes of the urea cycle. These are generally going to present in pediatric patients, but occasionally can present in adulthood as incomplete disorders may become clinically apparent under conditions of a stressor.
- Liver Disease: Both decreased liver function which can result in decrease of the urea cycle and bypassing the liver via a portosystemic shunt will result in elevated ammonia levels.
- Valproate toxicity
- Post lung transplant
AKI typically does not cause hyperammonemia by itself, but there will be aggravation with decreased renal clearance.
How Does Hyperammonemia Cause Toxicity?
With very high ammonia levels, ammonia crosses the blood brain barrier. In cerebral cells it is metabolized to glutamate which results in cellular swelling and cerebral edema.
Dialysis for Hyperammonemia
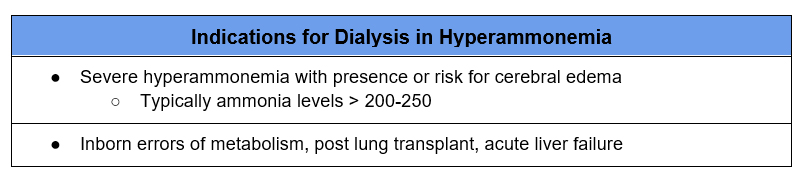
- Is hyperammonemia associated with significant morbidity or mortality?
- Severe elevations in ammonia are associated with cerebral edema in certain clinical situations. Levels > 250 are associated with brain herniation.
- Can ammonia be removed by dialysis?
- Ammonia can be removed by dialysis. It is small (molecular weight 17 daltons) and not protein bound. It does have a large volume of distribution so multiple treatments of intermittent or continuous renal replacement therapy is required to prevent rebound.
- Does removing ammonia with dialysis reduce morbidity or mortality?
- There is some evidence that dialysis improves outcomes, specifically 21 day transplant free all cause mortality.
In chronic liver disease, cirrhosis, cerebral edema from hyperammonemia is rare. Hepatic encephalopathy is multifactorial. But may be considered acute on chronic liver failure.
Dialysis Considerations
- Although intermittent dialysis can lower ammonia levels quicker, CRRT is typically used. That is because there is rebound given the high volume of distribution. Slower solute removal with CRRT also decreases the risk of cerebral edema.
- Higher dialysate effluent flow rates may be required to lower ammonia. (35 ml/kg/hr vs 20 ml/kg/hr).
- Maintain higher serum sodium. Therapeutic hypernatremia is a treatment for cerebral edema. If possible use a higher dialysate sodium concentration to target a serum sodium of 145 meq/L.
- Avoid alkalemia. With a high pH there is more ammonia (NH3) and less ammonium NH4+. The former more readily diffuses into brain cells. An increased serum HCO3– can also paradoxically cause a central nervous system acidosis. (HCO3– is converted to CO2 and CO2 more readily diffuses across the blood brain barrier). This intracerebral acidosis leads to vasodilation worsening cerebral edema. A standard dialysate necessary to correct metabolic acidosis with acute kidney injury may induce a metabolic alkalosis when kidney function is intact.
- Avoid hypophosphatemia. CRRT, especially if not associated with acute kidney injury, tends to be associated with hypophosphatemia.
- Continue renal replacement therapy ideally until clinical improvement and ammonia improves to < 150-200. If ammonia is controlled and there is no clinical improvement ongoing therapy may be futile.
- Monitor for rebound in ammonia levels after renal replacement therapy discontinued.
- Renal replacement therapy for hyperammonemia may be appropriate in acute liver failure even if the patient is not a candidate for transplant.
Summary
Severe hyperammonemia as may occur in acute liver failure or urea cycle disorders may be an indication for renal replacement therapy even if there is not associated kidney dysfunction.


{kind=link}
{kind=link}
{kind=link}