Table of Contents
Talking to patients and families regarding initiation of dialysis can be complex. Typically shared decision making is recommended. This involves more than simply asking if the patient “wants” dialysis.
There are two settings where this counseling is necessary. Each has different questions and concerns. The first is a patient with chronic kidney disease progressing towards End Stage Kidney Disease. This patient is typically seen in the outpatient setting. The second is a patient with Acute Kidney Injury (with or without chronic kidney disease). This patient may also be critically ill.
This article will address the patient with progressive chronic kidney disease in the outpatient setting.
When to have the Dialysis Discussion
Although it is always appropriate to have advance directive discussions, if the eGFR is < 20 the discussion should be had in most patients (if it has not been had already). There are two important reasons for this.
- When the eGFR is < 20 the patient can potentially be listed for a preemptive deceased donor kidney transplant and evaluated for a potential living donor transplant. Although the waitlist for a deceased donor transplant may be many years, the patient may be able to accrue time on the waitlist prior to dialysis initiation. This approach also allows time for the patient and potential donor to be evaluated and allows planning of a living related transplant when the eGFR is < 15, but prior to the need for dialysis.
- Dialysis access planning should occur when The Kidney Failure Risk Equation indicates a 2 year kidney failure risk of 20-40%. Most patients with an eGFR < 20 and overt albuminuria (albumin creatinine ratio > 300 mg/gram) will be in this range.
For patients with a more rapid CKD progression course (i.e. eGFR decreasing at a rate of > 5 ml/ minute/ year) and/or more severe proteinuria, it may be appropriate to initiate these discussions with the patient at a higher eGFR.
Patient Focused Concerns
- How long will I live with dialysis?
- How will dialysis make me feel?
There is not a straightforward answer to these questions. In general life expectancy is less and dialysis symptom burden higher with:
- Increasing age
- More comorbidities
- Frailty
How Long Will I Live With Dialysis?
Mortality for patients with ESRD maintained on dialysis has improved, but overall remains high. Below, I present United States Renal Data System (USRDS) Mortality data from 2019. (The mortality for patients with ESRD in 2020 was affected by COVID).
From a statistical patient population perspective mortality rate is expressed in deaths per 1,000 patient years. This data is not meaningful for most patients. I am not a statistician and therefore not sure if this is valid, but converting this to a death rate in percent per year may be more meaningful for a patient.
Hemodialysis
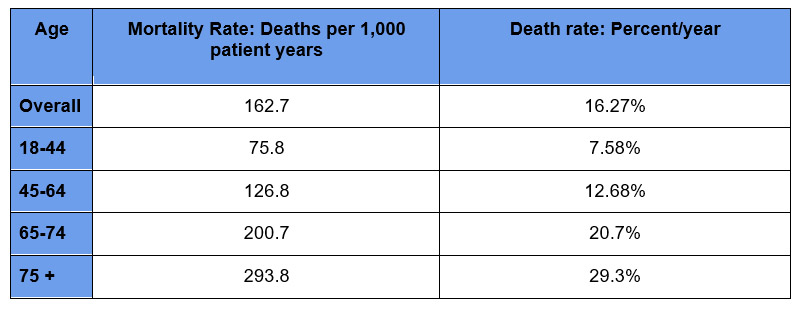
The mortality rates are lower for peritoneal dialysis. However this is because patients on peritoneal dialysis tend to be healthier.
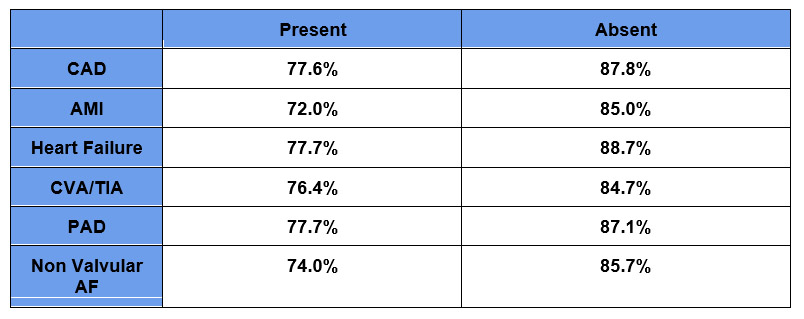
These are overall mortality rates for hemodialysis patients. The mortality rates are higher for patients with comorbidities. The USRDS Mortality report shows 12 month survival rates for the presence or absence of the following comorbidities.
This data can give the patient a general idea but more meaningful may be presenting the data as an average life expectancy. A pitfall here is that most people believe they will live longer than they will.
For this reason I put it in context of general life expectancy using social security actuarial data. Since social security is paying money they have a pretty good idea of how long people are going to live.
The below table contrasts 2019 social security life expectancy Actuarial Life Table with 2019 US Renal Data System (USRDS) hemodialysis life expectancy Mortality
Life Expectancy (How Many More Years of Expected Life) by Age
General Population vs Dialysis
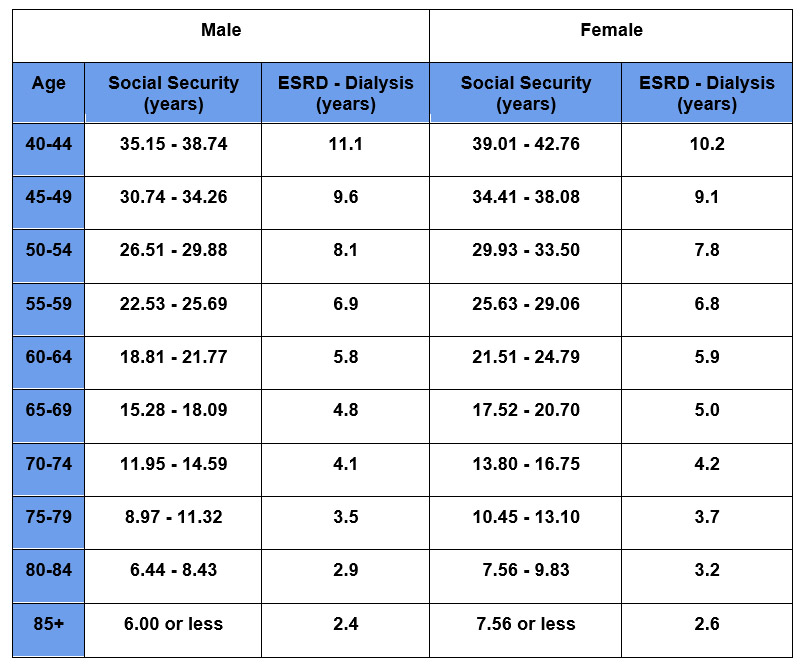
So a patient who is:
- 60 has an average life expectancy of about 6 years with dialysis
- 70 has an average life expectancy of about 4 years with dialysis
- 60 has an average life expectancy of about 3 years with dialysis
If the patient has AMI, CAD, Heart failure, AF, CVA/TIA, or PAD life expectancy would be shorter, if the patient has none of these conditions it will be longer.
For an older patient the benefit of dialysis given this life expectancy may need to be considered in context of the next question:
How Will Dialysis Make Me Feel?
Dialysis would be expected to improve uremic symptoms, however it comes with a symptom burden.
Improved uremic symptoms:
- Energy
- Appetite
- Dyspnea
- Volume overload
I take the following into context when counseling patients about what to expect regarding symptom improvement.
- GFR – Uremic symptoms become most prominent when the GFR is < 5-10. Symptoms that occur at this level I am confident will improve. When the GFR is higher > 15 or 10-15, there may be other nonuremic contributors to the patient’s symptoms. I counsel patients that these symptoms may only partially improve. Symptoms related to volume overload are an exception, they may improve at a higher GFR.
- Frailty – Symptoms related to frailty and functional capacity are likely to persist after dialysis initiation.
This study provides some insights. https://www.nejm.org/doi/full/10.1056/NEJMoa0904655
It examined nursing home patients who initiated dialysis. If we use nursing home status as a marker of frailty. It found that
- Within 3 months of starting dialysis 61% had died or had a decrease in functional status (when compared to pre dialysis).
- By 12 months 87% had died or had a decrease in functional status (when compared to pre dialysis).
Symptom burden:
- Fatigue
- Cramping
- Nausea
- Headaches
- Time commitment
The above symptom burden includes intradialytic symptoms (related to ultrafiltration and intradialytic hypotension). There is also a feeling of fatigue and being drained post dialysis requiring a post dialysis recovery time. For some this is relatively short (30 minutes or less), for others it may last the rest of the day. For these patients once they start feeling better it is time for their next dialysis.
I counsel patients that this occurs, but it is variable and difficult to predict what their specific symptom burden will be. In general the symptom burden is higher with increased age, comorbidities and frailty.
Pitfalls in the Dialysis Discussion
-
Pitfall # 1: Asking patients if they “want” dialysis.
Patients will often say they don’t want dialysis. Of course they don’t, no one “wants” dialysis. But, they don’t want to die either. When clarified they often say that they don’t want dialysis “if I don’t need it”. This can be an avoidance strategy which leads to pitfall # 2.
-
Pitfall # 2: Delayed planning.
Planning regarding dialysis modality choice (hemodialysis or peritoneal dialysis) and access (fistula) is important. Delays lead to an increased risk of emergent dialysis requiring hospitalization and temporary catheter access. I counsel patients to “ Hope for the best, prepare for the worst”.
-
Pitfall # 3: Categorizing the patient as “refusing” dialysis.
I don’t like this terminology. Non-dialysis treatment or Conservative Kidney Management is often a reasonable option. I counsel patients that we can continue medical treatments to help them feel as good as possible and live as long as possible, understanding that it would be expected to be shorter than if they did dialysis. For older patients the difference in life expectancy may be limited and in some studies Comparative Survival among Older Adults with Advanced Kidney Disease Managed Conservatively Versus with Dialysis it is not even clear that there is a survival advantage.
Summary
Counseling patients with CKD about dialysis can be difficult. For most patients I believe the discussions need to occur if the eGFR is < 20 especially if there is overt albuminuria. I use the available data to counsel on life expectancy and advise that symptoms that occur at a higher GFR or are related to frailty may not improve with dialysis. I encourage patients to be educated and follow through on pre dialysis planning. For some Conservative Kidney Care may be a good option.
For patient centered educational videos check out this link:
https://patient.health-ce.wolterskluwer.com/DART/programs

{kind=link}
{kind=link}
{kind=link}