Table of Contents
Kidney cysts are commonly found on imaging and are a common cause of anxiety for patients.
This overview will provide context with the aim of being able to minimize patient anxiety, avoid unnecessary referrals and triage patients for appropriate referral to nephrology or urology.
The main question to ask yourself when a kidney cyst or cysts are found is this. Is there something bad going on?
What’s bad?
- Kidney failure. Is there a condition that can lead to progressive CKD and kidney failure?
- Cancer. Is this malignant?
In most cases the answer to both is no. The most common renal lesion is a simple cyst. These are very common, and often found incidentally on imaging (US or CT scan).
Here are the questions to ask:
- Is the lesion a cyst or a mass?
- If it is a cyst: Is it simple or complex?
- If there is a cyst (or cysts) is there an underlying cystic kidney disease?
Is the Lesion a Cyst or a Mass?
Cyst – Fluid containing sac
Mass – Solid
Imaging can usually tell the difference. Occasionally the lesion will be described as indeterminate. These are typically < 1 cm, too small for the imaging to characterize.
Is the Cyst Simple or Complex?
What is a simple cyst?
It is a renal lesion that:
- Is round with smooth walls
- Contains only fluid (yellow/straw colored ultrafiltrate)
- Water density
- No internal echoes (anechoic)
- Good ultrasound through transmission
How common are simple cysts? Incidence on imaging (Ultrasound or CT)
- Overall incidence: 12-14%
- More common in males than females (@ 2:1)
- More common with increased age:
- Age < 15 – up to 12%
- Age > 50 up to 33%
Bottom line:
- Simple cysts are common
- Simple cysts are benign (not cancerous/malignant)
What is a Complex Cyst?
It is a cyst that has:
- Thickened or irregular walls.
- Internal septa
- Enhances with contrast
- Has a solid component
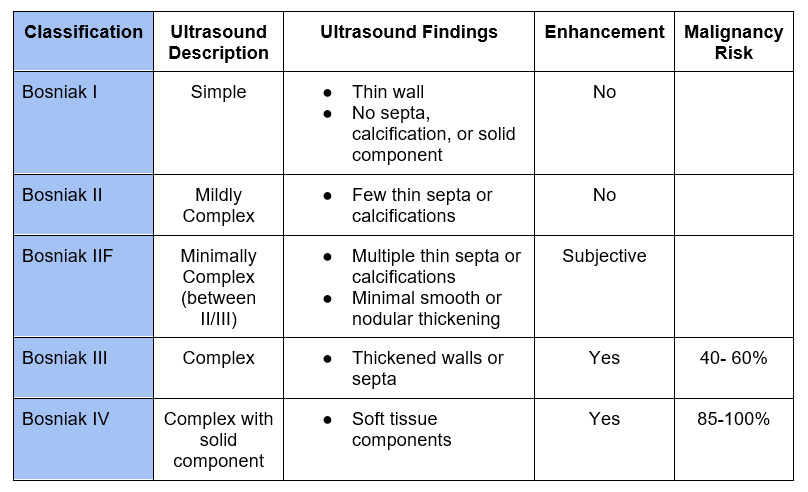
Most complex cysts will also be benign. There is a classification system to help stratify. It is referred to as the Bosniak classification.
The gist of the Bosniak classification is this: (This is a gross oversimplification – see below for more accurate information):
- Bosniak I: Definitely benign
- Bosniak II: Probably benign. Divided into:
- II: No need for surveillance
- IIF: Need for surveillance (F is for follow)
- Bosniak III: Probably cancer
- Bosniak IV: Definitely cancer.
I have only seen Bosniak II or IIF in radiology reports. More commonly the cyst will be described as: Simple, mildly/minimally complex, complex, or cyst with solid component.
Ok the Patient has Simple Cysts. Is there a Cystic Disease with Risk of Progressive Kidney Disease?
The questions to ask are:
- Is there a family history?
- Are the cysts multiple or bilateral (in a young patient – ie < 50)?
- Are the kidneys enlarged ?
- Are there other signs of kidney disease?
The list includes:
Autosomal Dominant Polycystic Kidney Disease (ADPKD) will be the most common.
- Autosomal Dominant. Most will have a positive family history. This is not 100%. Family history may be unknown or there may be a de novo mutation. Genetic testing is available.
- Multiple cysts (3 or more) in a young patient with family history of ADPKD is diagnostic.
- In ADPKD kidney failure develops because the renal parenchyma is replaced with cysts. The kidneys typically become enlarged in this process.
- An older patient (> 50) with decreased eGFR associated with a few cysts likely has another cause of CKD. However, a patient with decreased eGFR and multiple bilateral cysts may have another cystic kidney disease.
In addition to multiple benign simple cysts and Autosomal Dominant Polycystic Kidney Disease other cystic kidney conditions include:
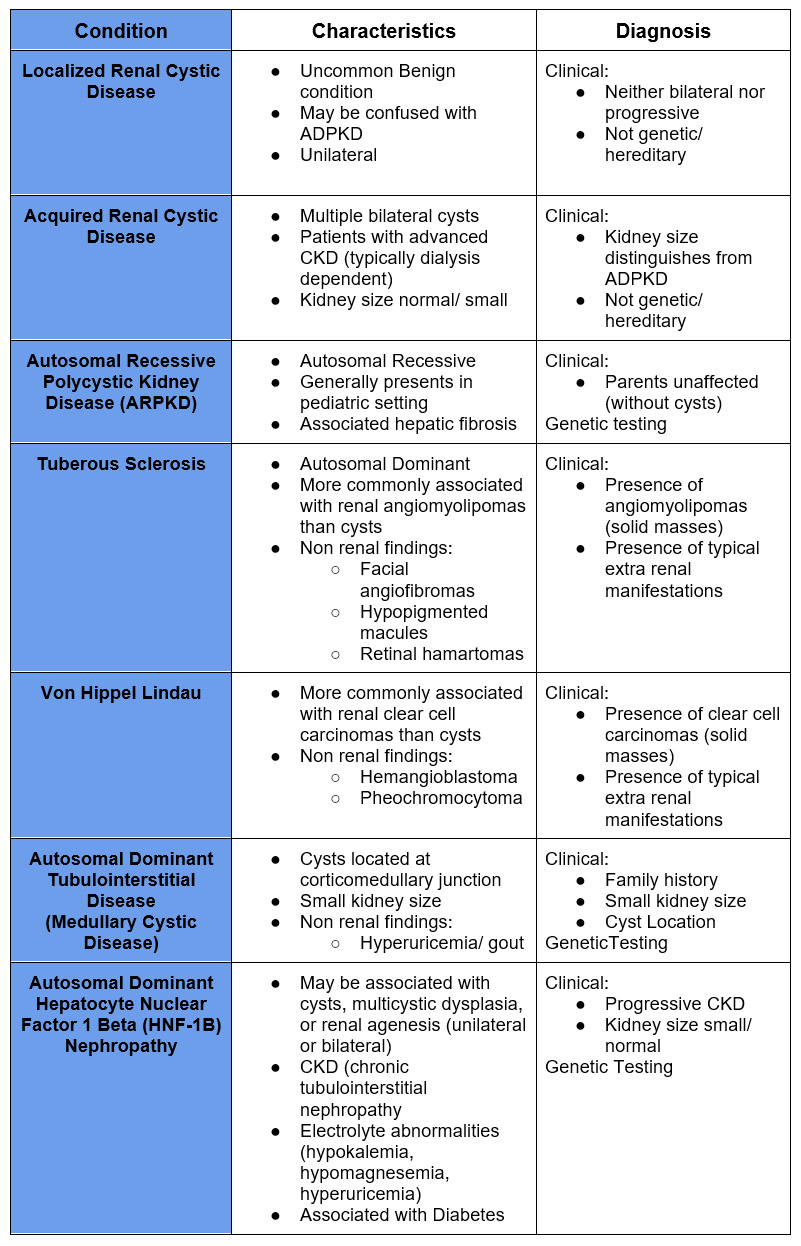
Some of these conditions may be rare, but I have made a diagnosis of Autosomal Dominant Hepatocyte Nuclear Factor 1 Beta (HNF-1B) Nephropathy. This was a patient with progressive CKD and bilateral cysts with normal sized kidneys and no family history of ADPKD. I performed a genetic screen/panel which showed this mutation.
Summary and Management
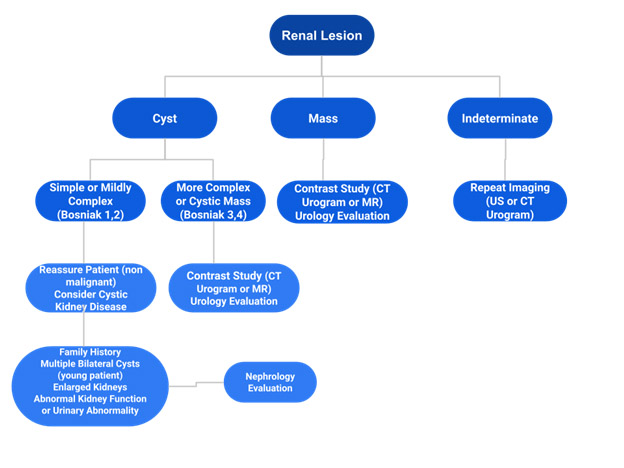
Is it a cyst , mass or indeterminate?
- Mass, more complex cyst (Bosniak III), or cyst with solid component (Bosniak IV)
- Contrast study CT urogram or MR with gadolinium
- Urology evaluation if:
- Unable to give contrast
- Enhancement on contrast study
- Indeterminate or Bosniak 2F
- Indeterminate: Follow up imaging (often with US or CT urogram)
- Bosniak 2F: Surveillance (6 months then yearly for 5 years)
- Simple cyst (Bosniak 1) or mildly complex (Bosniak 2)
- Reassure patient not malignant and no need for imaging follow up
- Screening questions for cystic kidney disease (see below)
Is there a Cystic Disease with Risk of Progressive Kidney Disease?
- Family history of ADPKD or other kidney disease
- Nephrology evaluation
- Multiple bilateral cysts in young patient
- Check eGFR and urinalysis
- Nephrology evaluation
- Multiple cysts with enlarged kidneys
- Consider genetic testing (for ADPKD)
- Nephrology evaluation
- Decreased eGFR or other signs of kidney disease
- Nephrology evaluation



{kind=link}
{kind=link}
{kind=link}