Table of Contents
What are the indications for Renal Replacement Therapy (RRT) with dialysis in Acute Kidney Injury (AKI)?
The common indications:
- Uremia
- Life threatening volume overload refractory to medical treatment
- Life threatening hyperkalemia refractory to medical treatment
- Life threatening metabolic acidosis refractory to medical treatment
- Life threatening intoxication with a dialyzable drug
This leaves the following questions:
- What about oliguria? Anuria?
- Does initiating RRT earlier improve prognosis/ outcomes
- What is life threatening? What is uremia?
There have been several studies that help provide clarity for practical management / decision making in the Intensive Care Unit (ICU) setting with stage 2 or 3 acute kidney injury (AKI). 3 of the 4 studies required stage 3 AKI. Practically this means:
- Creatinine either doubled (Stage 2 AKI) or tripled (Stage 3 AKI) or increased by at least 0.3 g/dl to a level > 4 g/dl (Stage 3 AKI).
Or
- Urine output was < 0.5 ml/kg/hr for 12 hours (Stage 2 AKI) or < 0.3ml/kg/hr for 24 hrs (Stage 3 AKI) or there was anuria for 12 hours (Stage 3 AKI).
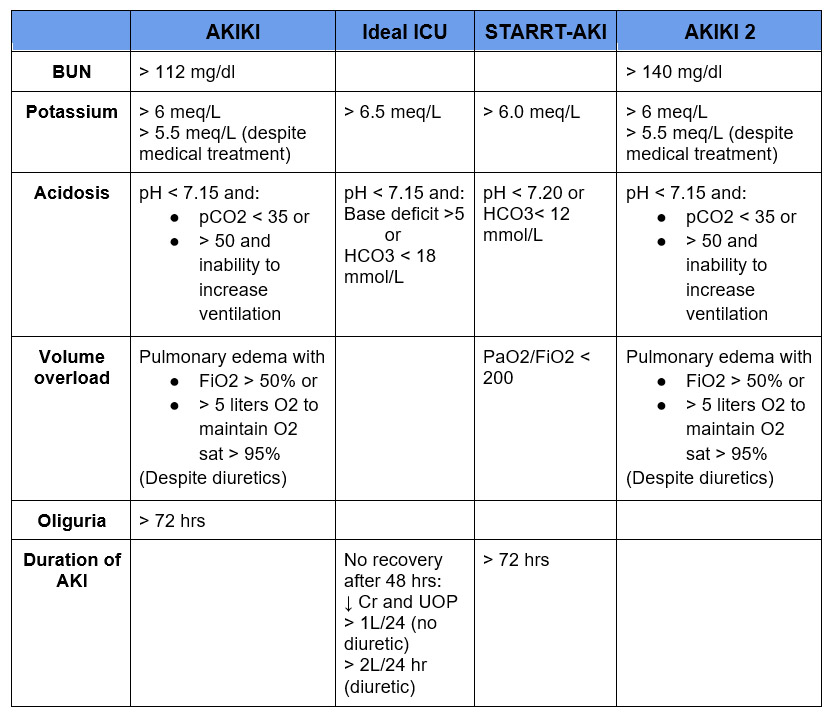
The Studies
AKIKI – Artificial Kidney Initiation in Kidney Injury
Initiation Strategies for Renal-Replacement Therapy in the Intensive Care Unit | NEJM
- Randomized trial of patients with ventilator and/or vasopressor requirement
- Early – within 6 hrs of diagnosis of stage 3 acute kidney injury.
- Delayed – Emergent indication (see table) or oliguria for > 72 hrs
- Outcomes:
- No difference in 60-day mortality (48.5 vs 49.7%)
- Delayed dialysis group:
- 49% did not require Renal Replacement Therapy (RRT)
- Diuresis returned earlier
- Less catheter bloodstream infections ( 5 vs 10%)
IDEAL-ICU
Timing of Renal-Replacement Therapy in Patients with Acute Kidney Injury and Sepsis | NEJM
- Randomized trial of patients with RIFLE Failure stage (Stage 3 AKI) and early vasopressor dependent septic shock (within 48 hours of vasopressor)
- Early RRT: within 12 hours of diagnosis
- Delayed RRT: Emergent indication (see table) or no recovery after 48 hrs
- Outcomes:
- Death at 90 days – no difference (58% vs 54%)
- 38% delayed did not require RRT
- 29% recovered
- 8% death
- 2% other
- 17% required emergent RRT
- More patients developed hyperkalemia in the delayed group ( 4% vs 0%) and there was a trend toward increased metabolic acidosis (17% vs 9% p = 0.07). Otherwise no significant difference in adverse events.
STARRT-AKI
Timing of Initiation of Renal-Replacement Therapy in Acute Kidney Injury | NEJM
- Randomized controlled trial of critically ill (ICU) patients with stage 2 or 3 acute kidney injury (AKI)
- Accelerated RRT initiation
- Within 12 hours of AKI diagnosis
- Standard RRT initiation
- Clinical judgment (Discouraged unless potassium > 6 meq/L, pH < 7.20, serum HCO3 < 12 mmol/L or PaO2/FIO2 < 200)
- AKI persisted for > 72 hours
- Outcomes
- No difference in mortality (death at 90 days) – 43.9% vs 43.7%
- Higher dependence on RRT for survivors (>90 days) in accelerated initiation group (10.4% vs 6.0%)
- More adverse events in the accelerated group (23% vs 16.5%).
- Mainly hypotension/ hypophosphatemia.
- No difference in severe adverse events (1.0% vs 0.5%)
AKIKI 2
Comparison of two delayed strategies for renal replacement therapy initiation for severe acute kidney injury (AKIKI 2): a multicentre, open-label, randomised, controlled trial – The Lancet
- Randomized controlled trial of patients in the delayed arm of AKIKI trial who did not require an urgent indication for RRT prior to endpoint (oliguria for 72 hrs or BUN > 112 mg/dl)
- Delayed
- Initiate RRT
- More delayed
- Delay RRT initiation until:
- Urgent indication (see table)
- BUN > 140 mg/dl
- Outcomes
- No difference in primary outcome (days alive without requiring RRT)
- Trend toward increased 60 day mortality
- 44 vs 55% (p= 0.071)
- Increased Hazard Ratio (multivariate analysis) for death (1.65)
- No difference in complications
- Delay RRT initiation until:
My Perspective
-
What about oliguria? Anuria?
- If you have oliguria or anuria long enough you will develop a life threatening indication (volume overload/ hyperkalemia) as there will be an inability to remove fluid and potassium.
- Oliguria by itself is not an indication to start RRT (for at least up to 72 hrs).
-
Does initiating RRT earlier improve prognosis/ outcomes
- Allowing 48-72 hours for AKI to recover is not associated with worse outcomes.
- But, delaying dialysis until BUN is > 140 mg/dl (in patients with AKI) may be associated with increased mortality.
-
What is life threatening?
- Potassium:
- > 6-6.5 meq/L
- Metabolic acidosis:
- pH < 7.15 – 7.20 and
- Depressed pCO2 or an inability to further ventilate or
- HCO3 < 18 or Base deficit > 5
- HCO3 < 12 mmol/L
- pH < 7.15 – 7.20 and
- Fluid overload/pulmonary edema.
- FIO2 >50% or PaO2/FiO2 ratio < 200 despite diuretics
- Potassium:
-
What is uremia?
- Findings severe enough to warrant dialysis initiation:
- Pericardial friction rub
- Unexplained myoclonus or seizures
- Other potential uremic findings (ie mental status changes, nausea, bleeding) are too nonspecific (if BUN is < 112-140 mg/dl).
- BUN elevation (if not associated with clinical findings is azotemia not uremia)
- Somewhere between 112-140 mg/dl. This is in patients with Acute Kidney Injury, not necessarily an indication for dialysis in patients without AKI.
- Findings severe enough to warrant dialysis initiation:
Summary
Delaying the initiation of dialysis for 48-72 hrs (in the absence of a potential life threatening indication) in patients with acute kidney injury is not associated with an increase in mortality. A significant percentage of these patients (approximately ⅓ – ½) won’t end up needing dialysis and will be able to avoid the potential complications associated with this invasive procedure. The above studies provide some practical guidelines as to what constitutes a life threatening indication. As always, clinical judgment should be used in each specific case.

{kind=link}
{kind=link}
{kind=link}
Thanks! Glad you found it helpful