Table of Contents
What Is Abiraterone?
Abiraterone (Zytiga) is a medication used in the treatment of metastatic prostate cancer. It works by decreasing the production of androgens in the testes, adrenal glands and the prostate tumor (androgen deprivation therapy).
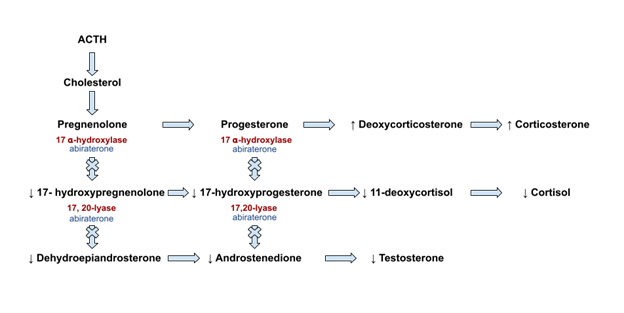
Abiraterone inhibits the enzyme Cytochrome P450 C17A1 (CYP17A1). This enzyme has two functions:
- 17𝝰-hydroxylase
- 17,20 lyase
Inhibition of this enzyme therefore decreases the activity of these 2 enzymes, which are necessary for the production of sex hormones.
- 17𝝰-hydroxylase is the first enzymatic step in the conversion of progesterone and
pregnenolone to active sex hormones.
- 20 lyase catalyzes the subsequent step in the production of androgens.
This is the same enzyme that is impaired in one of the variants of congenital adrenal hyperplasia,
How Does Abiraterone Cause Hypertension?
Abiratereone causes a syndrome of apparent mineralocorticoid excess, or pseudohyperaldosteronism. This is similar to hyperaldosteronism, but without the increased aldosterone. This results in:
- HTN
- Hypokalemia
- Metabolic alkalosis
How does this happen?
The conversion of progesterone and pregnenolone by 17𝝰-hydroxylase is also necessary for the production of cortisol, resulting in hypocortisolism.
- Hypocortisolism leads to a lack of suppression of ACTH
- ACTH levels increase
- Elevated ACTH levels leads to increased production of the glucocorticoid precursor
corticosterone and mineralocorticoid precursor deoxycorticosterone.
Despite hypocortisolism adrenal insufficiency does not occur because of the glucocorticoid activity from the increased levels of corticosterone.
Increased levels of deoxycorticosterone lead to increased mineralocorticoid activity resulting in the typical findings of HTN, hypokalemia and metabolic alkalosis seen in hyperaldosteronism.
Although aldosterone production is not dependent on 17𝝰- hydroxylase and therefore not affected by inhibition, the renin and aldosterone levels are typically low. This is because the volume expansion and hypokalemia caused by deoxycorticosterone suppress renin and aldosterone production.
Treatment of Abiraterone associated hypertension
Prednisone
- Abiraterone is always given concomitantly with low dose prednisone.
- Low dose prednisone suppresses ACTH release thereby decreasing production
of corticosterone and deoxycorticosterone.
- Initially the recommended dose of prednisone was 5 mg twice daily subsequently this
has been lowered to 5mg day
However a certain percentage of patients will still get hypertension despite prednisone.
Risk of Abiraterone associated hypertension with prednisone
- Prednisone 5mg day: 32.4%
- Prednisone 5 mg twice a day: 16.5%
(PDF) Risk of hypertension in Cancer patients treated with Abiraterone: a meta-analysis
Mineralocorticoid Antagonists
- Spironolactone is not recommended, as this is not selective for the mineralocorticoid receptor and can stimulate the androgen receptor, which is what treatment for prostate cancer is intending to avoid.
- The selective mineralocorticoid antagonist Eplerenone can be used.
Amiloride
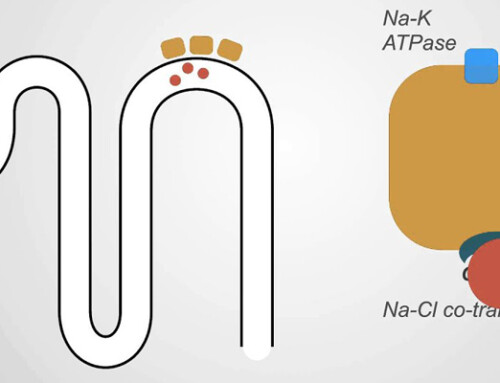
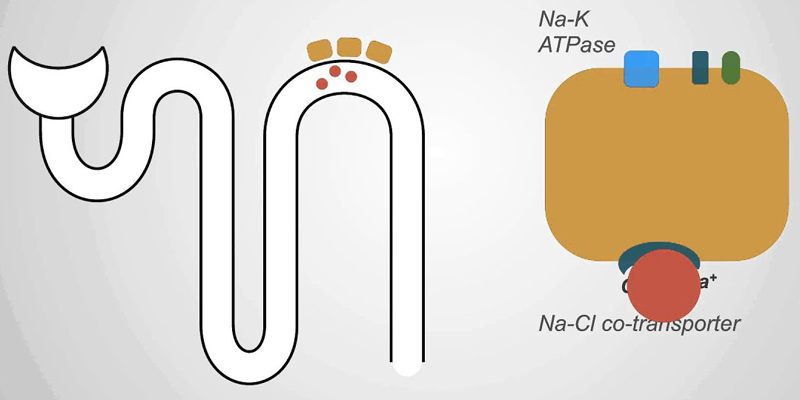
- The potassium sparing diuretic amiloride works by blocking the epithelial sodium channel (ENac) in the distal nephron. This channel is upregulated by activation of the mineralocorticoid receptor.
For an overview of diuretics check out this article: https://bcnephro.com/diuretics-an-overview/
Summary
In the patient with hypertension it is important to consider pre existing medications as a potential cause. In these cases discontinuation or substitution of the medication may result in resolution of the hypertension. In cases where the medication cannot be safely discontinued, understanding of the pathophysiology allows for the choice of effective antihypertensives and avoidance of medications that may interfere with the desired clinical effect.

{kind=link}
{kind=link}
{kind=link}